A 52 YEAR OLD FEMALE WITH DIABETIC KETOACIDOSIS
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 52 YEAR OLD FEMALE,TEACHER BY OCCUPATION, RESIDENT OF CHINTALCHERVU, SURYAPET, CAME TO THE OPD WITH C/O
PAIN ABDOMEN SINCE 5 DAYS.
VOMITING SINCE 9/8/21(5 days).
HEADACHE SINCE 5 DAYS .
DECREASED APPETITE SINCE 9 MONTHS.
H/O FEVER 5 DAYS BACK.
THE PATIENT WAS APPARENTLY ASYMPTOMATIC 9 MONTHS BACK , THEN SHE MET WITH AN ACCIDENT( FALL FROM A BIKE) AND FRACTURED DISTAL FEMUR OF RIGHT LEG WITH CLOSED INTRA ARTICULAR# WITH DIAPHYSIS EXTENSION PROXIMAL TIBIA , FOR WHICH SHE UNDERWENT Sx RIGHT ORIF WITH DISTAL FEMUR LOCKING PLATE WITH PROXIMAL TIBIAL LOCKING. SINCE THEN THE PATIENT HAD ON AND OFF FEVER(LOW GRADE) AND EPISODES OF VOMITING AFTER USING ANTIBIOTICS. HER VOMITING EPISODES SUBSIDED AFTER STOPPAGE OF MEDICATION.
H/O FROTHY URINE SINCE 1 MONTH, HEMATURIA SINCE 15 DAYS.
SINCE 5 DAYS PATIENT HAS PAIN ABDOMEN ( DIFFUSE TYPE) A/W VOMITING (BILIOUS), 10 EPISODES IN A DAY, FOLLOWED BY HEADACHE ( FRONTAL, NON RADIATING,NOT A/W BLURRING OF VISION), DIMINISHED VISION.
H/O FEVER 5 DAYS BACK (LOW GRADE FEVER)
NO DIURNAL VARIATION,SUBSIDED ON TAKING MEDICATION (DOLO).
SHE WENT TO THE LOCAL HOSPITAL, WHERE SHE WAS ADVISED FOR INVESTIGATION, WHICH SHOWED > RAISED SUGAR'S, AND WAS REFERRED TO OUR HOSPITAL.
PAST HISTORY
history of of Type 2 DM since 14 years.
NO H/O HTN/asthma /epilepsy/ TB.
She was operated in both eyes for cataract in 2018.
DRUG HISTORY -patient was on Glimi M2 in the intial years, where she complained of gaining excessive weight and hypoglycemia, then she was started on M1 , after which she complained of burning micturition, and now the patient is on Insulin( INJ.MIXTARD INSULIN 10U S/C OD).
PERSONAL HISTORY -
-diet mixed .
-decreased appetite .
-bowel and bladder movements: regular.
-no addictions.
- sleep: adequate.
FAMILY HISTORY - Mother is k/c/o Diabetes.
GENERAL EXAMINATION-
Patient is conscious, coherent and cooperative.
no pallor, icterus, no clubbing, no cyanosis, no lymphadenopathy,no edema.
Vitals-
PR-104 bpm.
BP-140/ 70 mm Hg.
RR-22 cpm.
Temperature-afebrile.
SpO2-98%
SYSTEMIC EXAMINATION-
CVS- S1, S2 heard, no murmurs, no added sounds.
RS- BAE+,NVBS heard, trachea central in position.
P/A- soft, non-tender, no palpable mass or swelling.
CNS- NAD.
PROVISIONAL DIAGNOSIS-
? DIABETIC KETOACIDOSIS
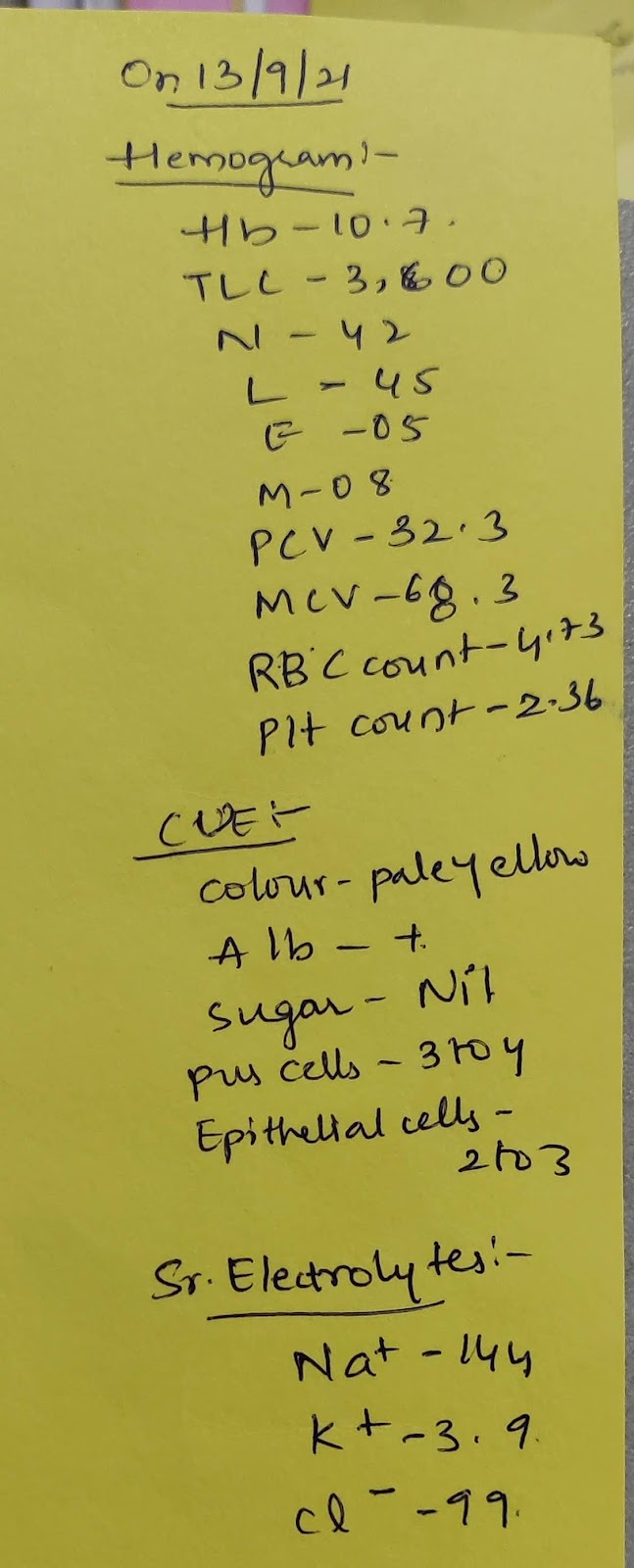
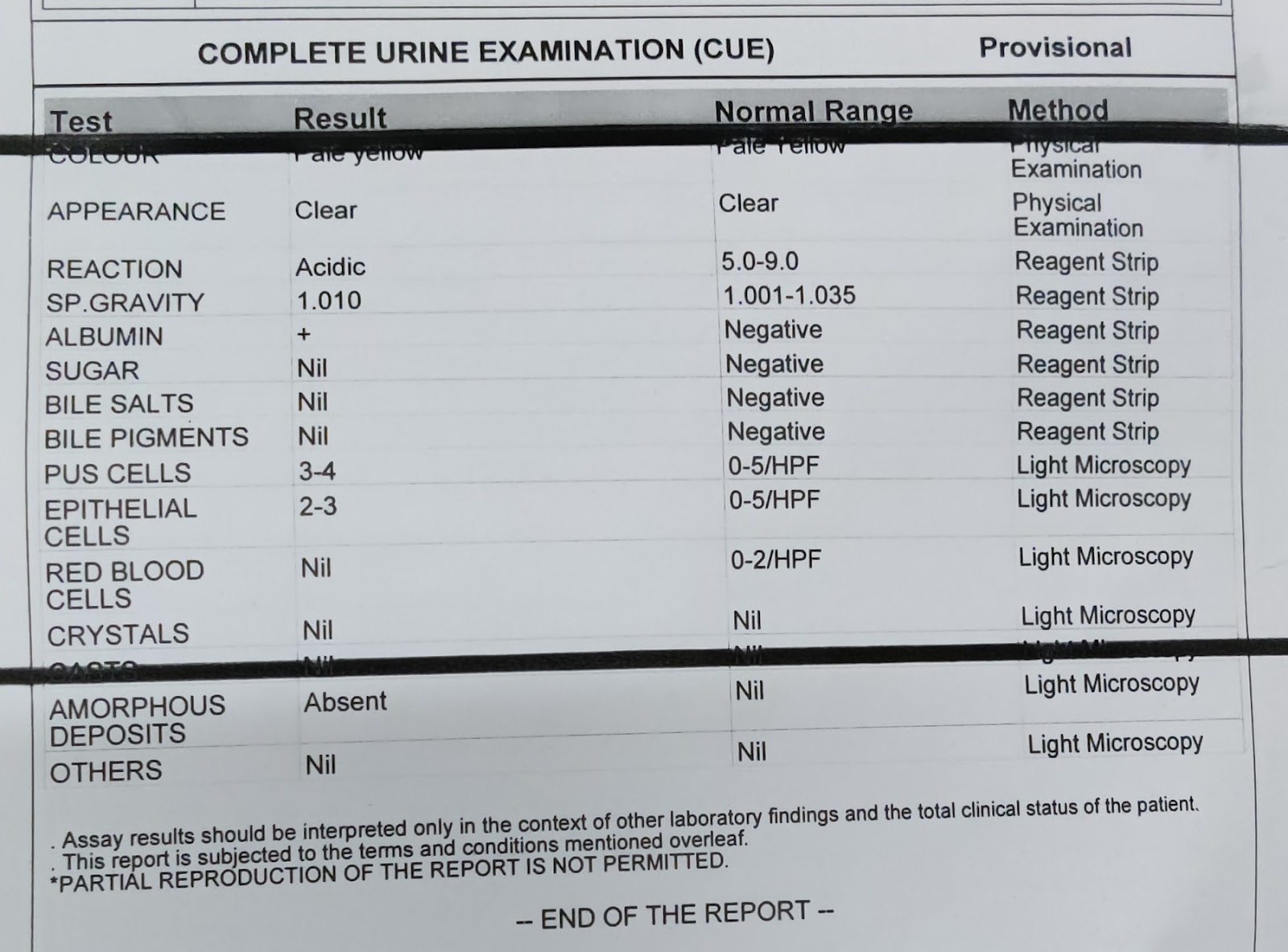
INVESTIGATIONS