A 35 year OLD FEMALE WITH HYPERTENSIVE URGENCY
This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.




This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
A 35 year old female r/o athmakuru came to the casualty for follow up i/v/o high bp.
FIRST VISIT
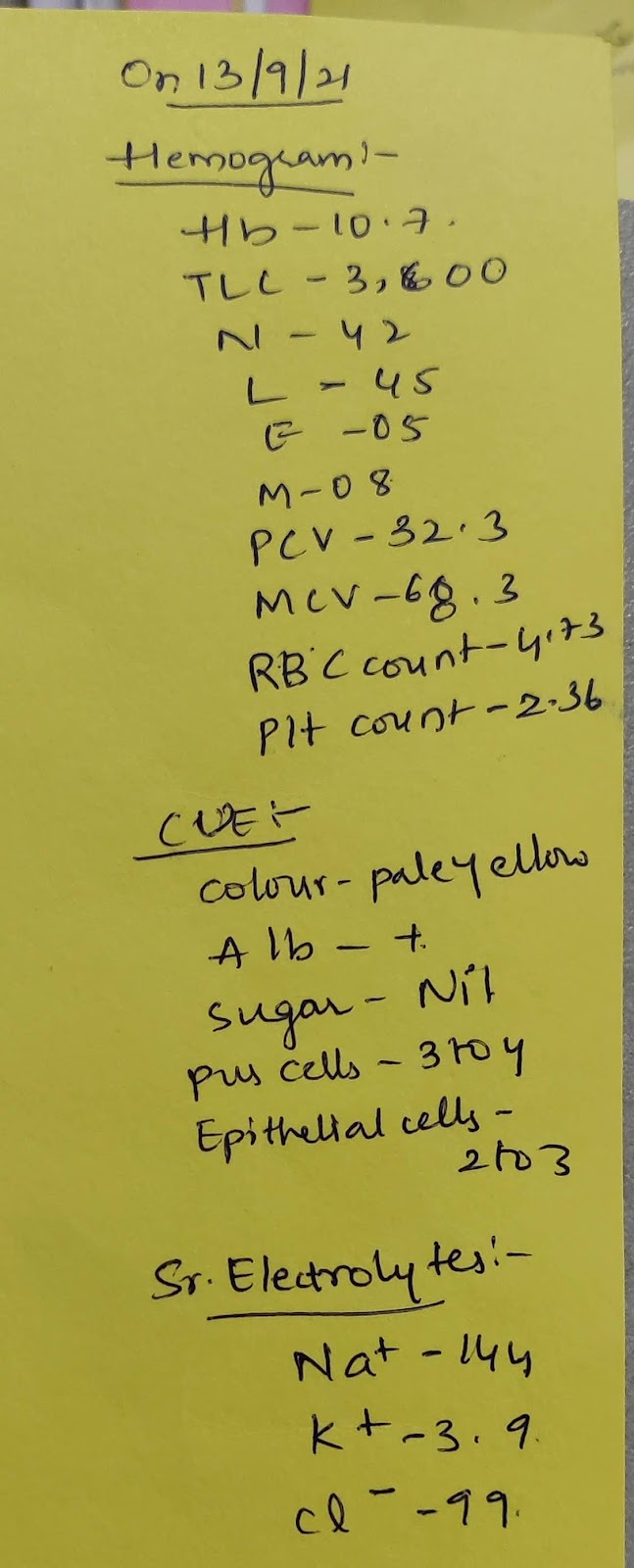
on 13/9/21 pt came with c/o fever a/w chills,cold,cough since 3 days( for which she consulted a local RMP, some injections were given , but the symptoms didn't subside so the patient came to our hospital)
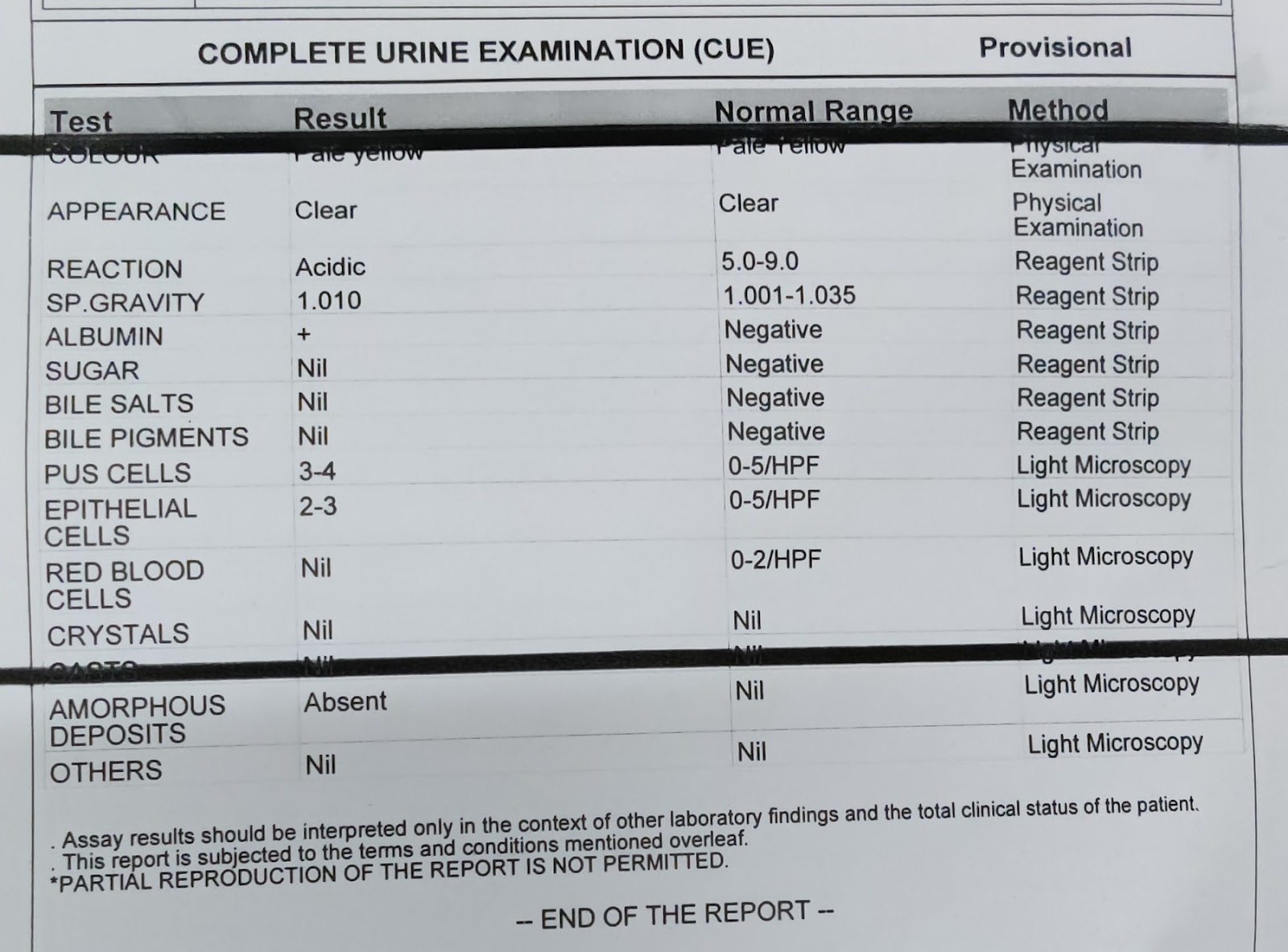
on examination her bp was 180/100 mmhg , advised T.Telma 20mg PO/OD and asked for regular bp monitoring at home (ECG showing LVH, Alb+ 2/1,Hb- 10.7,Tlc- 3600,plt-2.36)
Regular BP checkup was done ( which showed 180/100 170/100 mm hg alternatively).
Her Fever and other symptoms were reduced by medication, but as the patient had consistent high BP she was advised for a follow up after 1 week.
SECOND VISIT
ON 18/9/21
pt came for follow up i/v/o high bp (210/140 mmhg)
No E/O target on damage, no h/o blurring of vision , angina, reduced UO
Past History: H/O Gestational HtN 10 yrs back.
patient has 2 children.
1st pregnancy: 8th month> high BP> put on medication> normal delivery was done.
2 nd pregnancy: 8th month> high bp> was put on medications> LICS was done.
No H/O DM,TB, Epilepsy, Thyroid.
No other surgeries were done.
O/E
Pt is c/c/c.
moderately built and nourished
Temp: Afebrile.
BP: 230/140 mmhg.
PR: 88bpm.
RR: 20 Cpm.
CVS :s1s2 heard.
RS: BLAE+, NVBS
P/A : Soft,non tender
CNS: NAD.
DIAGNOSIS
HYPERTENSIVE URGENCY.
PRIMARY ALDOSTERONISM UNDER EVALUATION
TREATMENT GIVEN
initially T.NICARDIA 20 mg PO STAT was given when BP was 210/10 mm hg.
later in the evening when her
BP raised to 240/130 mm hg
INJ.LABETOLOL 10 mg Iv STAT given.
now her blood pressure has decreased to 160/100 mmhg and is on
TAB. TELMA-AM (40/5) PO/OD.
INVESTIGATIONS



OPHTHALMOLOGY REFERRAL: In view of any fundus changes( Hypertensive Retinopathy) was done, which revealed Normal Fundus.









SOAP NOTES
DAY 1
Subjective- No New Complaints
Objective:
pt is c/c/c
BP: 160/100 MM HG
PR:78 bpm.
Temp: Afebrile.
Assessment: HYPERTENSIVE URGENCY.
Plan of care:
TAB. TELMA- AM (40/5) PO/OD.
BP monitoring hourly.
DAY 2
Subjective- No New Complaints
Objective:
pt is c/c/c
BP: 190/110 mm hg
PR:86 bpm
Temp: Afebrile
Assessment: HYPERTENSIVE URGENCY.
Plan of care:
TAB. TELMA- AM (40/5) PO/OD.
BP monitoring hourly.
Took Telma 20 mg at 10 am, her bp was 140/90 then. @ 19/9/21.
She took TELMA AM (40/5) at 8 am 20/9/21.
SOAP NOTES DAY 3
A 35 Year old female came i/v/o High BP.
S- No New Complaints
O-
pt is c/c/c
BP:
Rt UL: 160/100 mm hg
Lt UL:180/110 mm hg
Rt LL:200/120 mm hg
Lt LL:200/110 mm hg.
PR:96 bpm.
Temp: Afebrile
Diagnosis: Hypertensive Urgency.
Plan of care:
TAB. TELMA- AM (40/5) PO/BD.
Tab.HYDROCHLORTHIAZIDE 12.5 mg PO/OD
BP monitoring hourly.
SOAP NOTES DAY 4
A 35 Year old female came i/v/o High BP.
S- No New Complaints
O-
pt is c/c/c
BP:
Rt UL: 170/110 mm hg
Lt UL:180/110 mm hg
Rt LL:190/120 mm hg
Lt LL:190/110 mm hg.
PR:84 bpm.
Temp: Afebrile
Diagnosis: Hypertensive Urgency.
Plan of care:
TAB. TELMA- AM (40/5) PO/BD.
Tab.HYDROCHLORTHIAZIDE 12.5 mg PO/OD
BP monitoring hourly.
SOAP NOTES DAY 5
A 35 Year old female came i/v/o High BP.
S- No New Complaints
O-
pt is c/c/c
BP:
Rt UL: 160/110 mm hg
Lt UL:170/110 mm hg
Rt LL:160/100 mm hg
Lt LL:150/100 mm hg.
PR:84 bpm.
Temp: Afebrile
Diagnosis: Hypertensive Urgency.
Plan of care:
TAB. TELMA- AM (40/5) PO/BD.
Tab.HYDROCHLORTHIAZIDE 12.5 mg PO/OD
T.ANXIT 0.25 mg PO/OD (8pm)
BP monitoring hourly.
http://keerthykasa80.blogspot.com/2021/09/a-35-year-old-female-with-hypertensive.html
SOAP NOTES DAY 6
A 35 Year old female came i/v/o High BP.
S- No New Complaints
O-
pt is c/c/c
BP:
Rt UL: 140/100 mm hg
Lt UL:140/110 mm hg
Rt LL:150 mm hg
Lt LL:150 mm hg.
PR:84 bpm.
Temp: Afebrile
Diagnosis: Hypertensive Urgency.
Plan of care:
TAB. TELMA- AM (40/5) PO/BD.
Tab.HYDROCHLORTHIAZIDE 12.5 mg PO/OD
T.ANXIT 0.25 mg PO/OD
(8pm)
T.Aldactone 50 mg PO/OD ( 2 pm)
BP monitoring 2 nd hourly.
DAY 7
A 35 Year old female came i/v/o High BP.
S- No New Complaints
O-
pt is c/c/c
BP:
Rt UL: 140/100 mm hg
Lt UL:140/100 mm hg
Rt LL:140 mm hg
Lt LL:150 mm hg.
PR:84 bpm.
Temp: Afebrile
Diagnosis: Hypertensive Urgency.
PRIMARY ALDOSTERONISM UNDER EVALUATION
Plan of care:
TAB. TELMA- H PO/BD.
T.AMLONG 5 mg OD(2pm)
T.Aldactone 50 mg PO/OD ( 2 pm)
BP monitoring 2 nd hourly.
DISCUSSION POINTS:
Approximately 90-95% of adults with hypertension have primary hypertension, whereas secondary hypertension accounts for around 5-10% of the cases. [11] However, secondary forms of hypertension, such as primary hyperaldosteronism, account for 20% of resistant hypertension (hypertension in which BP is >140/90 mm Hg despite the use of medications from 3 or more drugs (1 of which is a thiazide diuretic).
25% of patients with primary aldosteronism can have normal Potassium .
Primary aldosteronism (15-20%) is commoner than pheochromocytoma (0.6%)
http://emedicine.medscape.com/article/241381-overview
What is the most sensitive and specific test to go by and is their sensitivity and specificity worth the money that we shall spend on the test, knowing well that medical management will only consist in aldosterone blockers that can be added anyways?
These proportion of patients with normal Potassium ,found to have aldosterone producing adenoma .
And two most common cause of sporadic primary aldosteronism is adrenal adenoma and bilateral adrenal hyperplasia .They account for more than 90 % cases.
Screening test - plasma aldosterone to Renin ratio - 90% sen ,91% specificity
For the levels of aldosterone more than 20 ng / ml
And ratio more than 30:1
https://pubmed.ncbi.nlm.nih.gov/16509213/
And after this what imaging would have the highest sensitivity and specificity?
Retrospective analysis of 187 patients .
7 patient had - normal Potassium .
More than 2/3 rd patients had adrenal adenoma .(135 pt)
All patients underwent CT abdomen for adrenal adenoma / hyperplasia .
The ratio of plasma aldosterone concentration (ng/dl) to plasma renin activity (ng/ml/h) was above 20 in all patients with aldosterone-producing adenoma .
The PPV of adrenal imaging was 97.6% for NCS, 85.0% for CT scan (P=0.04) and 83.3% for MRI (P=0.03), and the sensitivity was 85.4%, 85.0% and 74.1%, respectively (P=NS)
https://pubmed.ncbi.nlm.nih.gov/12766605/
High resolution CT may diagnosis tumor as small as 0.3 cm ,PPV-90% .
If non diagnostic -
Adenoma may be detected by adrenal scintigraphy after dexamethasone suppression test ,but sensitivity is decreased of tumor size less than 1.5 cm .
For unilateral aldosterone secretion Sens and specificity of adrenal venous sampling -95 and 100 %
Superior to CT abdomen
Reminds us about one of our previous long distance patients who was missed elsewhere till we got it both on imaging as well as biochemistry
but if it's adrenal adenoma and if surgery done this refractory hypertension can be controlled?
That patient with a large adrenal adenoma is still in our follow up, normotensive on medications alone
Its curative in 40-70 % of patients
Revisiting our previous patient's case report here
http://globaludhc07.blogspot.com/2015/12/a-50-years-old-woman-with.html?m=1
She was undiagnosed for 18 years .
Yes imagine!
most of them are not diagnosed .
But she did well for 18 years ,not symptomatic also .